

Umbilical Cord
 The umbilical cord (also called the birth cord or funiculus umbilicalis) is the connecting cord between the developing embryo or fetus to the placenta. Developed from the same zygote as the fetus, the umbilical cord normally contains two arteries (the umbilical arteries) and one vein (the umbilical vein), buried within Wharton's jelly. The umbilical vein supplies the fetus with oxygenated, nutrient-rich blood from the placenta. Conversely, the umbilical arteries return the deoxygenated, nutrient-depleted blood.
The umbilical cord (also called the birth cord or funiculus umbilicalis) is the connecting cord between the developing embryo or fetus to the placenta. Developed from the same zygote as the fetus, the umbilical cord normally contains two arteries (the umbilical arteries) and one vein (the umbilical vein), buried within Wharton's jelly. The umbilical vein supplies the fetus with oxygenated, nutrient-rich blood from the placenta. Conversely, the umbilical arteries return the deoxygenated, nutrient-depleted blood.
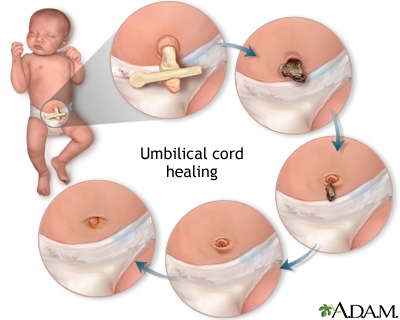
Shortly after birth, upon exposure to temperature change, the gelatinous Wharton's Jelly substance undergoes a physiological change that collapses previous structure boundaries and in effect creates a natural clamp on the umbilical cord which halts placental blood return to the neonate, causing the cord to cease pulsation. This process will take as little as five minutes if left to proceed naturally.
Problems and abnormalities
A number of abnormalities can affect the umbilical cord, which can cause problems that affect both mother and child:
• Nuchal cord
• Single umbilical artery
• Umbilical cord prolapse
• Umbilical cord knot
• Umbilical cord entanglement
• Vasa previa
• Velamentous cord insertion
Nuchal cord
A nuchal cord occurs when the umbilical cord becomes wrapped around the fetal neck 360 degrees.
Diagnosis
Doppler ultrasound has been successfully used to identify a Nuchal cord, and also to determine the orientation of the loop.
Prognosis and treatment
Nuchal cord can be managed by home fetal monitoring. It doesn't have a higher risk of birth complications. About 1 in 3 babies have the umbilical cord wrapped around their neck at the birth.
Cutting the umbilical cord should not be done until it has stopped pulsating (upwards of 20 minutes after birth). In the case of a nuchal cord the child is still receiving blood and oxygen to the brain. As always the umbilical cord should not be cut until it ceases to pulsate (after all the blood from the placenta has been sent to the child.)
Checking for the presence of a nuchal cord is the second step in delivering a newborn in the pre-hospital setting. During a cephalic delivery, after the head presents the first step is to support the head and then use the middle finger to check for the presence of a nuchal cord. If one is discovered, an attempt to unwrap the cord is made. If the nuchal cord is wrapped too tightly around the newborns neck and cannot be corrected, it is clamped in two places and carefully cut to relieve the tension, preventing strangulation and other complications.
Single Umbilical Artery
Occasionally, there is only the one single umbilical artery (SUA) present in the cord. Approximately 1 in 100 newborns are found to have a SUA, making it the most common umbilical abnormality. It is more common in multiple births. Babies with SUA may have a higher likelihood of having other congenital abnormalities. However, additional testing (high level ultrasound scans) can rule out many of these abnormalities prior to birth and alleviate parental anxiety. Echocardiograms of the fetus may be advised to ensure the heart is functioning properly. Genetic counseling may be useful, too, especially when weighing the pros and cons of more invasive procedures such as chorionic villus sampling and amniocentesis.
It is important to note that a diagnosis of SUA, while anxiety provoking, is in no way a guarantee that a fetus is at risk for other problems in utero or after birth. Especially encouraging are cases in which no other soft markers for congenital abnormalities are visible via ultrasound. Prior to ultrasound technology, the only method for determining the presence of a SUA was at birth, following an examination of the placenta. Given that the vast majority of expectant mothers do not receive the kind of advanced ultrasound scanning required to confirm SUA in utero, most cases may never be detected antenatally even today.
Doctors and midwives often suggest parents take the added precaution of having regular growth scans near term to rule out intrauterine growth restriction, which can happen on occasion and warrant intervention. Yet the majority of growth restricted infants with the abnormality also have other defects. Finally, neonates with the finding may also have a higher occurrence of kidney problems, so close examination of the infant may be warranted shortly after birth. Among SUA infants, there is a slightly elevated risk for post-natal urinary infections.
Umbilical cord prolapse
Umbilical cord prolapse is an obstetric emergency during pregnancy or labour that endangers the life of the fetus. It occurs when the umbilical cord presents itself outside of the uterus while the fetus is still inside. It can happen when the water breaks – with the gush of water the cord comes along. Usually, thereafter the fetus will engage and squash the cord, cutting off oxygen supplies and leading to brain damage of the fetus, or stillbirth. Before that happens, the baby must be delivered quickly by caesarean section. In the meantime, the woman adopts the knee-elbow position, and an attendant reaches into the vagina and pushes the presenting part (usually the head) back in so that it does not suffocate the cord. It is useless to try to push the cord back in.
The mortality rate for the fetus is given as 11-17%. This applies to hospital births or very quick transfers in a first world environment. One series is reported where there was no mortality in 24 cases with the novel intervention of infusing 500ml of fluid by catheter into the woman's bladder, in order to displace the presenting part of the fetus upward, and to reduce compression on the prolapsed cord.
Vasa praevia
Vasa praevia (vasa previa) is an obstetric complication defined as "fetal vessels crossing or running in close proximity to the inner cervical os. These vessels may be from either a velamentous insertion of the umbilical cord or may be joining an accessory (succenturiate) placental lobe to the main disk of the placenta. If these fetal vessels rupture the bleeding is from the fetoplacental circulation, and fetal exsanguination will rapidly occur, leading to fetal death.
Diagnosis
• This is rarely confirmed before delivery but may be suspected when antenatal sono-gram with color-flow Doppler reveals a vessel crossing the membranes over the internal cervical os.
• The diagnosis is usually confirmed after delivery on examination of the placenta and fetal membranes.
• Most often the foetus is already dead when the diagnosis is made; because the blood loss (say 300ml) contitutes a major bulk of blood volume of the fetus (80-100ml/kg i.e. 300ml approx for a 3kg foetus).
Treatment
Treatment immediately with an emergency cesarean delivery is usually indicated.
Velamentous cord insertion
In velamentous cord insertion, the umbilical cord inserts in the chorion rather than in the mass of the placenta. The exposed vessels are not protected by Wharton's jelly and hence are vulnerable to rupture.
